

Mayors' Conferences
- Details
- Category: The ECAD Mayors' Conference
- Published: 27 May 2016
Following is a rough summary compiled by ECAD of the main points from some of the presentations. For in depth information about the presentations or the publications featured download the slides or contact the speakers directly.
The conference participants were welcomed by the Chairman of Rogeland County Council Solveig Ege Tegnesdal and the vice mayor of Stavanger Bjørg Tysdal Moe.

Building healthy and safe cities through prevention and treatment
The first Key note speaker was Mr. Raymond Yans, Member of the International Narcotics Control Board (INCB) and its former chair between the years 2012-2014. In his speech Building healthy and safe cities through prevention and treatment, Mr. Yans emphasized the role of demand reduction and prevention as cost efficient and effective efforts to counteract the economic and social consequences of drug abuse and save government costs later on.
He urged all ECADs member cities to continue sharing knowledge and best practices of the effectiveness of prevention measures in various contexts and to undertake prevention strategies that are comprehensive, sustainable and based on the common grounds reflected in the drug control conventions.
The full speech by Mr Raymond Yans can be read here.
International Standards of Drug Use Prevention
Following Mr Yans speech, United Nations Office on Drugs and Crime (UNODC) Programme Officer Wadih Maalouf, PhD gave us a comprehensive overview of the International Standards of Drug Use Prevention that the UNODC has developed. The primary objective of prevention is to help people (particularly-not exclusively-young people) avoid or delay initiation of use, or, if they started already, to avoid to develop disorders (e.g. dependence). The general aim is much broader. It is the healthy and safe development of children and youth to realize their talents and potential, becoming contributing members of their community and society.
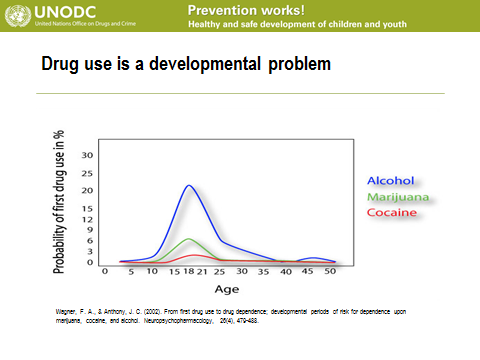
Each stage of development, from infancy to early adulthood, is associated with a certain expected range of:
- intellectual ability
- language development
- cognitive, emotional and psychological functioning
- social competency skills
Each needs attention to prevent the onset of drug use and dependence.
Interventions Based on Scientific Evidence are designed to prevent initiation and escalation of drug use and related problems among children who are exposed to risk conditions and experiences and who have personal characteristics that heighten risk:
- To overcome adversity
- Increase resiliency skills
- Reduce the level of exposure to deleterious factors
Believed to exert effects through improvements in:
- Underlying brain and cognitive functions
- Corresponding skill sets
- Underlying mental health, emotional and behavioral problems

Well-grounded in science on prevention, the standards identifies common characteristics among prevention programmes designed for different age groups and gives an overview over what works and what does not in prevention.
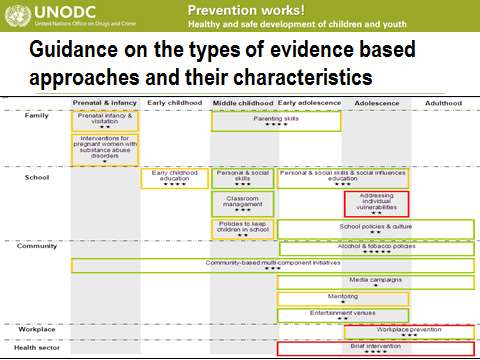
For more information on the UNODCs standards on drug use prevention read the slides by Mr Waidh Maalouf or download the standards.
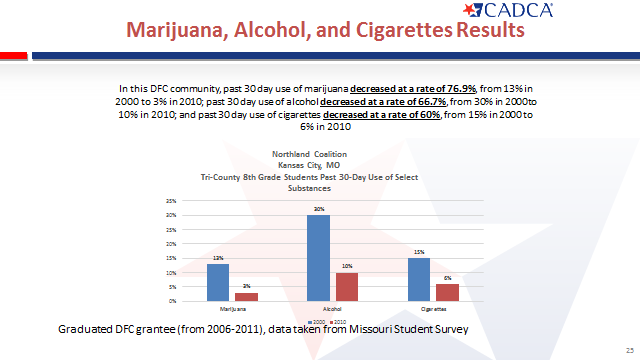
Effective Drug Prevention: CADCA’s Community Coalition Model
Sue Thau, Public Policy Consultant at CADCA (Community Anti-Drug Coalitions of America)
Download Sues presentation here
CADCA was founded in 1992 as a recommendation from the President’s Drug Advisory Council. Today, CADCA supports a comprehensive, data-driven approach to prevent the use of illicit drugs, underage drinking, youth tobacco use, and the abuse of medicines representing more than than 5,000 community coalitions.
CADCA’s Vision is a world of safe, healthy, and drug-free communities.
CADCA´s mission is to strengthen the capacity of community coalitions to create and maintain safe, healthy, and drug-free communities globally
Keys to Pushing Back Against Drug Use
- Taking a comprehensive, data-driven approach that appropriately mobilizes those who have a role in reducing access to and availability of drugs
- Changing social norms about the harms that drug use can cause is also critical
Coalitions
A coalition is a formal arrangement for cooperation and collaboration between groups or sectors of the community, in which each group retains its identity but all agree to work together towards a common goal of building a safe, healthy, and drug-free communit
Coalitions bring together community sectors to develop and carry out data-driven, evidence-based strategies to achieve population-level reductions in substance abuse rates to include underage drinking, tobacco use, illicit drug use, prescription drug and OTC misuse and abuse


The Health & Social Effects of Nonmedical Cannabis Use - The State of Knowledge: Knowns & Unknowns
Department of Mental Health & Substance Abuse WHO HQ Geneva
Presented by Mr Dag Rekve
What follows is a shortened version presentation of the report.
The full presentation can be downloaded here.
The report of non-medical use of cannabis is produced by the WHO and can be downloaded here
The report is about:
- nonmedical use of cannabis, not medical use.
- the health and social effects of cannabis use.
- the current knowledge on a very broad impact on health; “what we know”.
- priority areas for future research; where we lack sufficient knowledge.
The report is the outcome of two years of work and was developed by a broad range of scientists, medical doctors, experts that provided background papers in their area of expertise. An expert meeting was held to discuss and review the evidence. A smaller group drafted the report led by three main editors. The work was reviewed by external reviewers.
The report covers:
- Cannabis substance profile and its health impact.
- Neurobiology of cannabis use.
- Short-term effects of cannabis.
- Mental health and psychosocial outcomes of long-term cannabis use.
- Long-term cannabis use and non-communicable diseases.
- Prevention: interventions targeting families, school settings, vulnerable groups.
- Treatment of disorders: therapies, management of acute cannabis intoxication and withdrawal, relapse prevention.
How has WHO judged the evidence?
First requirement: Evidence of an association between cannabis use and the health outcome
Second requirement: Evidence that makes reverse causation an implausible explanation of the association. To rule out that cannabis use is a consequence of the health outcome rather than the cause of it.
Third requirement: Most difficult, to assess evidence that the association is not explained by other uncontrolled or unmeasured factors (as cannabis users are likely to use other drugs, and of the difference from non-users in risk-taking etc.).
Fourth requirement: A causal relationship between cannabis use and the health outcome is biologically plausible
Other factors that may support a causal interpretation include strength of the association, dose–response relationships, specificity of the association and reversibility of the effect after removal of the drug.
How have WHO defined the harms to health?
WHO has looked at the severity of the effects do to:
- The properties of the substance itself
- The form and mode of administration used
- The characteristics of the person taking the substance
- The social context in which it is taken
What we know about the short-term effects of cannabis use
The most obvious short-term health effect of cannabis is intoxication marked by disturbances in the level of consciousness, cognition, perception, affect or behaviour, and other psychophysiological functions and responses.
A minority of first-time cannabis users become very anxious, have panic attacks, experience hallucinations and vomit. These symptoms may be sufficiently distressing to prompt affected users to seek medical care.
Acute use impairs driving and contributes to an increased risk of traffic injuries.
There is some evidence that cannabis use can trigger coronary events. Recent case reports and case series suggest that cannabis smoking may increase CVD risk in younger cannabis smokers who are otherwise at relatively low risk.
What we know about the long-term effects of regular cannabis use
Regular cannabis users can develop dependence on the drug. The risk may be around 1 in 10 among those who ever use cannabis, 1 in 6 among adolescent users, and 1 in 3 among daily users.
Withdrawal syndrome is well documented in cannabis dependence.
Growing evidence reveals that regular, heavy cannabis use during adolescence is associated with more severe and persistent negative outcomes than use during adulthood.
In a number of prospective studies there is a consistent dose−response relationship between cannabis use in adolescence and the risk of developing psychotic symptoms or schizophrenia.
The association between cannabis use and psychosis or schizophrenia has been recognized for over two decades in at least four ways:
- Cannabis produces a full range of transient schizophrenia-like positive, negative and cognitive symptoms in some healthy individuals.
- In those harbouring a psychotic disorder, cannabis may exacerbate symptoms, trigger relapse and have negative consequences on the course of the illness
- With heavy cannabis use, susceptible individuals in the general population develop a psychotic illness which is associated with age of onset of use, strength of THC in the cannabis, frequency of use and duration of use.
- Cannabis use is associated with lowering the age of onset of schizophrenia It is likely that cannabis exposure is a "component cause" that interacts with other factors to precipitate schizophrenia or a psychotic disorder, but is neither necessary nor sufficient to do so alone.
Long-term cannabis smoking produces symptoms of chronic and acute bronchitis, as well as microscopic injury to bronchial lining cells, but it does not appear to produce COPD.
Long-term heavy cannabis smoking can potentially trigger myocardial infarctions and strokes in young cannabis users.
Smoking a mix of cannabis and tobacco may increase the risk of cancer and other respiratory diseases but it has been difficult to decide whether cannabis smokers have a higher risk, over and above that of tobacco smokers.
There is suggestive evidence that testicular cancer is linked to cannabis smoking and this potential link should be investigated further.
What we know about prevention and treatment
Evidence-based preventive interventions should cover the whole prevention chain from universal and selective to indicated prevention.
Comprehensive family prevention that involves training for parents, children and the family collectively is found to be effective in reducing both lifetime cannabis use and past-year use in adolescents.
Life skills programmes that combine both a social competence curriculum and social influence approaches are shown to reduce cannabis use at 12-month follow-up and beyond.
Interactive social programmes targeting vulnerable young people is found to be effective in reducing past-month cannabis use.
A single-session brief psychological intervention of 30−45 minutes increases the chances of cannabis cessation if people are not dependent on cannabis.
Many people with cannabis-use disorders cease cannabis use without treatment.
For people who are dependent on cannabis, family interventions are effective for adolescents, and CBT, MET and PPS are effective in adults.